Research In Practice Blog

Helping Parents Quit Smoking
A new study published in the journal Pediatrics investigated how researchers from Children’s Hospital of Philadelphia (CHOP), University of Pennsylvania, and Massachusetts General for Children have successfully and effectively integrated an automated tobacco treatment system to increase maternal smoking cessation rates significantly. This innovation, implemented across 12 practices in the CHOP primary care network, uses iterative quality improvement (QI), electronic health record (EHR) design, and change management strategies.
It is well known that parental smoking is a leading source of secondhand smoke exposure for children, increasing risks of respiratory illness and future smoking. Therefore, helping parents quit smoking is a longstanding public health priority, and primary care pediatricians are well-positioned to help these patients and their caregivers. Yet cessation treatment delivery for parents remains rare in pediatrics. To address this problem, researchers developed and evaluated a study titled “An EHR-based tobacco treatment system for parents in pediatric primary care” to assess the population-level impact of an automated tobacco treatment system integrated into the electronic health record (EHR) in pediatric primary care. This work builds upon findings from a prior study published in JAMA Network Open in September 2025.
Study Design and Findings
Researchers, including Clinical Futures Core Faculty members Brian P. Jenssen, MD, MSHP; Janani Ramachandran, MS, MPH; Jeritt Thayer, PhD; Robert W Grundmeier, MD; Tyra Bryant-Stephens, MD; and Alexander G. Fiks, MD, MSCE conducted an NIH-funded cluster-randomized controlled trial (RCT) in twelve pediatric primary care practices from June 2021–Aug 2024.
- Six practices used an automated, EHR linked pre-visit questionnaire offering screening, motivational messaging, and opt-out treatment (home-delivery of nicotine replacement therapy and connection to ongoing counseling through SmokefreeTXT and/or the Quitline).
- Six used screening only.
This analysis included all parents who completed questionnaires during routine care, excluding parents enrolled in the trial. Researchers analyzed self-reported cessation rates among parents who reported smoking during the study period.
“We developed this innovation to help parents stop smoking and in turn reduce children's exposure to secondhand smoke and improve health outcomes. Through this analysis of the data after integration, we hope to show the success of our innovation and the ability for it to be implemented across health system nationwide,” said Dr. Brian Jenssen, the lead study author and Associate Director for Clinical Impact at Clinical Futures, at CHOP.
EHR-Linked System: Direct Screening
The graphic below provides an example of the EHR-Linked System and how researchers accomplished direct screening.
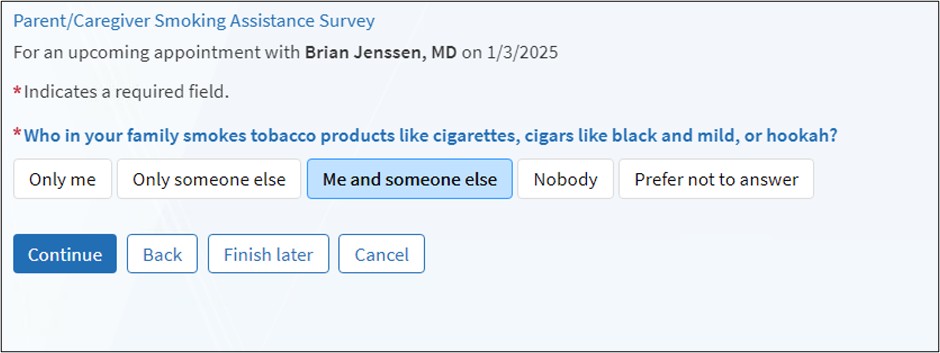
Source: Jenssen BP et al. Electronic Health Record-Embedded, Behavioral Science-Informed System for Smoking Cessation for the Parents of Pediatric Patients. Appl Clin Inform. 2022.
Results
Among 55,567 parents with follow-up data, smoking rates were lower in practices with the system: 4.3% of mothers smoked compared to 5.5% in practices without the system, and 6.5% of fathers smoked compared to 8.3% in non-system practices. For mothers who smoked during the study, the rates of cessation at follow-up were significantly higher when the system was in place: 37.4% compared to 33.5% (p=0.044), resulting in a 3.9% absolute improvement. In contrast, there was no difference in cessation rates among fathers, which remained the same at 29.6% for both groups.
The sample size for fathers was substantially smaller (n=436) compared to mothers (n=2,399), they had significantly shorter follow-up periods at system practices, and they completed fewer questionnaires overall. These factors limited the statistical power and opportunities to observe cessation among fathers. Additionally, the pediatric healthcare setting may be more effective in engaging mothers than fathers in treatment. Mothers are often the primary healthcare decision-makers for children and tend to attend pediatric visits more frequently, which creates more opportunities for treatment engagement and stronger motivation to respond to cessation messages focused on child health. In contrast, fathers attend fewer pediatric visits and may feel less connected to the clinical environment, which could reduce their receptiveness to interventions provided through their child's healthcare system.
“Pediatric settings can be used not only to assess the health of children but to connect with parents and advocate for healthy lifestyles. We know millions of parents who smoke attend visits with their children. Integrating this innovation into the pediatric setting can help reach those parents, thereby protecting children from secondhand smoke. This innovation is also cost-effective for the hospital and designed to integrate seamlessly into the Electronic Health Record (EHR), accumulating nearly a zero marginal cost. Furthermore, each parent who quits not only reduces their lifetime healthcare costs but also decreases the risk of their children developing future smoking habits and respiratory diseases,” said Dr. Jenssen.
With millions of parents who smoke attending pediatric visits annually, even small improvements in cessation rates can lead to tens of thousands of additional individuals who quit each year, thereby protecting hundreds of thousands of children from secondhand smoke exposure. From a cost-effectiveness perspective, automated systems incur nearly zero marginal costs per additional person reached once implemented in the Electronic Health Record (EHR), making modest increases in effectiveness quite valuable.
What’s Next? Research in Practice Implications:
These findings have significant implications for both practice and policy. They demonstrate the feasibility and effectiveness of addressing maternal smoking in pediatric settings through automated systems. The lack of effectiveness observed for fathers suggests that different or additional approaches may be necessary. Healthcare systems should not assume that interventions that are effective for mothers will automatically work for fathers.
“The successful implementation of this system highlights the potential for similar strategies to be broadly utilized in reducing children's exposure to secondhand smoke. It is important; however, these strategies may need to be tailored to each gender to maximize their impact on the community. By adopting this scalable approach, we can significantly enhance pediatric preventive care and decrease tobacco use within households, leading to healthier environments for our children,” said Dr. Jenssen.
Information & Resources:
- A Clinical Decision Support System for Motivational Messaging and Tobacco Cessation Treatment for Parents: Pilot Evaluation of Use and Acceptance
- Electronic Health Record-Embedded, Behavioral Science-Informed System for Smoking Cessation for the Parents of Pediatric Patients
- Automated Smoking Interventions Offered to Parents through Pediatric Primary Care May Curb Their Tobacco Habits | Children's Hospital of Philadelphia
- Take Down Tobacco National Day of Action: Celebrating CHOP’s Tobacco Treatment Platform in Primary Care | | Clinical Futures
- Clinical Conversations with Dr. Brian Jenssen: Tackling Tobacco Use in Adolescents | | Clinical Futures
Clinical Futures author(s): Brian P. Jenssen, MD, MSHP, Jan Ramachandran, MS, Jeritt Thayer, PhD, Robert W Grundmeier, MD, Tyra Bryant-Stephens, MD, Alexander G. Fiks (co-senior)
Additional authors: Abra M. Jeffers, PhD, Emara Nabi-Burza, PhD, Bethany Hipple Walters, PhD, Douglas E. Levy, PhD, Olivier Drouin MDCM MSc MPH, Mark Vangel, PhD, Nancy A. Rigotti, MD, Jonathan P. Winickoff (co-senior)
This study was funded by the NIH grant number, R01-CA245145.