Research In Practice Blog

The number of children hospitalized with pulmonary embolism tripled from 2001-2014, according to data from the Pediatric Health Information Systems (PHIS). Pulmonary embolism (PE) occurs when a blood clot blocks and stops blood flow to a pulmonary artery in the lung. This can be life-threatening. Treatment includes anticoagulants, clot-dissolving medications (thrombolytics), or surgical intervention. While cases of PE are increasing, within individual centers, pediatric PE remains relatively rare.
“As pediatric PE is rare, it is challenging for all potentially involved healthcare providers to develop expertise in PE management,” said Hilary Whitworth, MD, MSCE, a Clinical Futures Core Faculty member and the primary investigator on a new study to investigate PE management and treatment.
Creating standardized evaluation, management and treatment plans for this high-risk, low-frequency event can help coordinate care across clinical specialties with the potential to significantly improve clinical outcomes and patient well-being. With adult patients, the use of pulmonary embolism response teams (PERTs) has led to decreased hospital stay, decreased mortality, and increased utilization of advanced therapies. The International Society on Thrombosis and Haemostasis Subcommittee on Pediatric and Neonatal Thrombosis and Hemostasis had recommended that institutions create protocols to standardize pediatric PE management.
Implementation of a PE clinical pathway and PE response team (PERT)
“The establishment of a Pediatric PE Clinical Pathway and PERT at CHOP aims to standardize evaluation, improve multidisciplinary care coordination, minimize time to anticoagulation, and enhance patient outcomes,” said Dr. Whitworth.
The clinical pathway and PE response team were implemented at CHOP from September 2022 to August 2024. The aims of PERT include:
- Standardize patient evaluation and risk stratification
- Enhanced coordination across specialties
- Minimize time to anticoagulation
- Increased availability of advanced therapies and
- Standardized outpatient follow-up
For intermediate or risk high cases, the hematology fellows activate the PERT team and coordinate a virtual PERT call. The call includes the primary team caring for the patient, a PERT hematologist with expertise in PE, and the on-call attendings and fellows for hematology, general cardiology, interventional cardiology, and the PICU. Cardiac surgery, interventional radiology (IR), diagnostic radiology, and the echocardiography cardiologist join the call, as needed. This call isintended to occur within 30 minutes of activation, and the team discusses the risk and benefits of available therapies and creates management plans. The PE clinical pathway also includes a structed follow-up plan with a specific cardiologist identified to see all patients with intermediate and high-risk PE, in addition to hematology follow up for anticoagulation management.
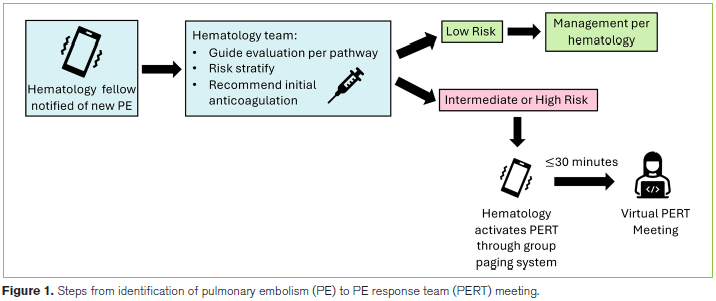
Following implementation of the PE clinical pathway there were 33 patients with acute PE compared to 175 episodes pre-pathway. The PERT was successfully activated for seven patients with 6 intermediate- and 1 high-risk PE. The median time from PERT activation to PERT call meeting was 30 minutes.
Improved Evaluation and Rapid Multidisciplinary Care
The development and implementation of this PE clinical pathway and PE response team led to improved standardizations of PE evaluation and provided rapid multidisciplinary care for intermediate and high-risk PE. Post-pathway, there was an increase in number of patients with BNP measured, troponin measured, and patients who had an echocardiogram during their admission. There were no significant changes in length of stay or time to reperfusion therapy.
Initial process outcomes show increased standardized evaluations with echocardiograms and laboratory testing, though further analysis is needed to assess long-term impacts on outcomes such as length of hospital stay and mortality.
“Our goal with this report was to provide an example of the development of a feasible, structured process to provide care for this high-risk, low-frequency pediatric disease,” said Michael O’Byrne MD, MSCE, a co-author on the study who helped develop the pathway and pulmonary embolism response team.
“We believe that pediatric-specific evaluation and management algorithms and PERTs provide standardization and a collaborative approach that will improve outcomes,” said Dr. Whitworth.
By implementing PERTs, hospitals can facilitate faster, coordinated responses to pediatric PE, potentially reducing time to treatment and improving survival rates. Involving trainees in PERT activations helps build expertise in PE management, which is crucial given the rarity of the condition.
Hilary B. Whitworth, MD, MSCE, Catherine M. Avitabile, MD, Michael L. O'Byrne, MD, MSCE
Whitworth HB, Wagner KM, Avitabile CM, Blowey B, Costello RA, Davis JC, Davis DH, Ellison AM, Giglia TM, Himebauch AS, Houng K, Law CK, Mavroudis CD, Mercer-Rosa L, O'Byrne ML, Ravishankar C, Raffini LJ. Development, Implementation, and Evaluation of a Pediatric Pulmonary Embolism Clinical Pathway and Pulmonary Embolism Response Team. Pediatr Crit Care Med. 2025 Oct 17. doi: 10.1097/PCC.0000000000003841. Epub ahead of print. PMID: 41104902.